

의료 감수: 박석민 한의사 (대표원장)
척추관절염(spondyloarthritis, SpA) 강직성척추염의 개요
목차
허리 통증이 좀처럼 가라앉지 않는다면, 척추관절염(SpA)을 의심해봐야 할까요?

척추관절염(spondyloarthritis, SpA)은 척추와 말초관절의 염증을 중심으로 포도막염, 손가락염(dactylitis), 건선(psoriasis) 등이 함께 나타나며 HLA-B27 유전자와 깊이 연관된 질환군입니다. 단일 질병이 아니라 여러 유사 질환을 아우르는 범주이며, 그 안에서 가장 잘 알려진 것이 강직성 척추염(AS)입니다. 이 글에서는 척추관절염의 분류와 유병률, 주요 증상, 그리고 예후까지 핵심만 정리해 보겠습니다.
척추관절염은 어떻게 분류되나요
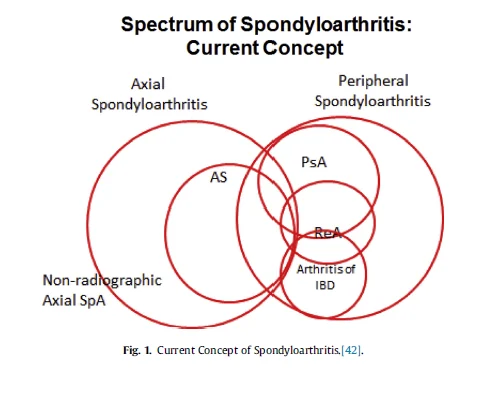
척추관절염은 침범 부위를 기준으로 크게 두 갈래로 나뉩니다. 임상 양상이 서로 일정 부분 겹친다는 점이 진단을 어렵게 만드는 특징이기도 합니다.
- 축형 척추관절염(Axial SpA) — 척추와 천장관절 중심
- 강직성 척추염(Ankylosing Spondylitis, AS)
- 비방사선학적 축형 척추관절염(Non-radiographic axSpA)
- 말초형 척추관절염(Peripheral SpA) — 팔다리 관절 중심
- 건선관절염(Psoriatic arthritis, PsA)
- 반응관절염(Reactive arthritis, ReA)
- 염증성장질환 관련 관절염(IBD-associated arthritis, IBDA)
아래 그림은 2014년 국제척추관절염평가학회(Assessment of SpondyloArthritis International Society, ASAS)에서 제안한 척추관절염 분류 체계입니다. 이 분류는 Raychaudhuri와 Deodhar가 J Autoimmun(2014)에 정리한 진단 기준을 토대로 합니다.
얼마나 흔한 질환인가요 (유병률·발생률)
유병률은 민족과 지역에 따라 차이가 큰 편입니다. 같은 질환이라도 조사 집단에 따라 수치가 크게 달라집니다.
- 네덜란드 조사: 약 0.1%
- 노르웨이 조사: 1.1~1.4%
- 종합적으로는 0.1% vs 2.5% 범위로 다양하게 보고됩니다.
이 중 강직성 척추염만 떼어 보면 0.1~1.4%의 유병률을 보입니다. van der Linden 등(Arthritis Rheum 1984)은 HLA-B27 양성자에서의 발병 위험을 일반 인구와 비교해 보고한 바 있습니다.
발생률은 지난 50여 년간 거의 일정하게 유지되어 왔습니다.
- 미국: 인구 10만 명당 7.2명
- 핀란드: 인구 10만 명당 6.9명
- 노르웨이: 인구 10만 명당 7.26명
Bakland와 Nossent(Curr Rheumatol Rep 2013)는 척추관절염의 역학을 종합적으로 검토하며 이러한 일관된 발생률 양상을 정리했습니다.
어떤 증상이 나타나나요
증상은 관절에 국한된 것과 관절 바깥으로 퍼지는 것으로 구분됩니다.
관절 증상
- 천장관절염 — 엉치엉덩관절의 염증
- 척추염으로 인한 등통증 — 환자의 약 70%가 경험
- 말초관절염 — 하지, 특히 무릎과 발목을 잘 침범하며 비대칭적으로 1~3개 관절을 동시에 침범
- 부착부염(enthesitis) — 인대·건·관절낭·근막의 염증으로, 발뒤꿈치 부착부염이 가장 흔함
- 손발가락염
관절 바깥 증상
- 포도막염 — 전방포도막염(홍채염)이 급성·편측으로 발생(약 20%)하며 수개월 지속되고 50% 이상에서 재발. 치료에 실패하면 영구 시력 장애로 이어지기도 합니다(Rosenbaum, J Rheumatol 1989).
- 건선
- 염증성 장질환 — 내시경 검사상 절반 이상에서 장 염증 소견이 보고됩니다(De Vos 등, Gastroenterology 1989).
- 심혈관 증상 — 강직성 척추염 환자의 2~10%에서 대동맥 역류, 1~9%에서 심전도 전도 이상이 관찰됩니다(Bergfeldt, Ann Intern Med 1997).
- 폐 증상 — 폐 실질 침범이 1~2%에서 나타나며 상엽 섬유화, 균종(mycetoma) 형성, 흉막 비후도 동반될 수 있습니다(El Maghraoui & Dehhaoui, Pulm Med 2012).
- 신장 증상 — 신장 아밀로이드증이 4~9%에서 나타나고, IgA 신증과 약물성 신독성도 주의해야 합니다(Nabokov 등, Nephrol Dial Transplant 1996).
예후는 어떤가요
강직성 척추염은 발병 후 10~15년 이내에 약 70%에서 척추 강직이 진행된다는 보고가 있습니다(Barkham 등, Ann Rheum Dis 2004). 또한 일반 인구와 비교했을 때 사망률이 1.5~4배 높게 나타나며, 40세 이상에서는 생존율이 10% 이상 감소하는 것으로 알려져 있습니다.
사망의 주요 원인으로는 심혈관 질환(가장 흔함), 뇌혈관 질환, 악성종양, 신부전, 폐렴, 자살 등이 꼽힙니다. Zochling과 Braun(Clin Exp Rheumatol 2008)은 사망 위험도가 질환의 활동성과 밀접하게 연관된다는 점을 강조했습니다. 즉 염증 활성도를 꾸준히 관리하는 것이 예후를 좌우합니다.
다른 관절염에서 강직성 척추염으로 진행할 수 있나요
척추관절염은 처음의 진단명이 끝이 아니라, 시간이 지나며 다른 형태로 이행하기도 합니다.
- 건선관절염 환자의 약 25%, 염증성장질환 관련 관절염 환자의 10~20%에서 방사선학적 천장관절염이 나타납니다.
- 반응성 관절염 환자의 약 20%가 강직성 척추염으로 진행합니다(Sieper 등, Best Pract Res Clin Rheumatol 2006).
- 미분화 척추관절염 환자의 약 24%가 강직성 척추염으로 진행합니다(Sampaio-Barros 등, J Rheumatol 2010).
따라서 초기 증상이 모호하더라도 경과를 꾸준히 추적 관찰하는 것이 중요합니다.
인천 송도 이레한의원은 강직성 척추염을 비롯한 자가면역질환을 오랜 기간 진료하며, 환자 한 분 한 분의 염증 활동성과 전신 증상을 함께 살피는 데 집중하고 있습니다. 척추 통증뿐 아니라 포도막염, 장 증상, 피부 증상까지 전체 그림을 이해하는 것이 관리의 출발점이라고 봅니다.
⚠️ 본 글은 의학 정보 제공을 목적으로 하며, 정확한 진단·치료는 전문 의료기관에서 받으시기 바랍니다.
자주 묻는 질문
Q. 척추관절염과 강직성 척추염은 같은 병인가요?
A. 같지 않습니다. 척추관절염(SpA)은 여러 유사 질환을 아우르는 큰 범주이고, 강직성 척추염(AS)은 그 안의 축형 척추관절염에 속하는 대표적인 한 유형입니다. 이 외에도 건선관절염, 반응관절염, 염증성장질환 관련 관절염 등이 같은 범주에 포함됩니다.
Q. 허리 통증이 있으면 모두 척추관절염을 의심해야 하나요?
A. 그렇지는 않습니다. 다만 척추관절염에 의한 등·허리 통증은 환자의 약 70%가 경험하며, 염증성 요통은 휴식해도 잘 나아지지 않고 새벽이나 아침에 뻣뻣함이 심해지는 특징이 있습니다. 이런 양상이 수개월 이상 지속된다면 전문 의료기관 평가가 필요합니다.
Q. 척추관절염은 관절 외에 다른 장기에도 문제를 일으키나요?
A. 그렇습니다. 포도막염(홍채염), 염증성 장질환, 대동맥 역류 같은 심혈관 증상, 폐 섬유화, 신장 아밀로이드증 등 관절 바깥 증상이 동반될 수 있습니다. 그래서 관절 증상만이 아니라 전신을 함께 살피는 접근이 중요합니다.


